
Last week, I had the chance to teach a kettlebell cert with Sarah Smith. I have thought for awhile that some (too much!) of our teaching needs a review. The biggest gap seems to be, and I can’t overstate this, is training women. And this is most clear when it comes to issues of the pelvic floor.
-Dan John.
When we exert ourselves to complete a task in real life or the gym, we use our breath to help create and slowly release intra-abdominal pressure (IAP) to generate tension and make us more powerful.
In the kettlebell world, we refer to this as the hardstyle or tension breath.
The act of breathing is the coordination of a TEAM of players comprised of the diaphragm, core and pelvic floor.
If you think of your core as a canister,
the top of the core is the diaphragm, a muscle that moves downward during the inhale to allow air to enter the lungs and moves upward on the exhale to push air out.
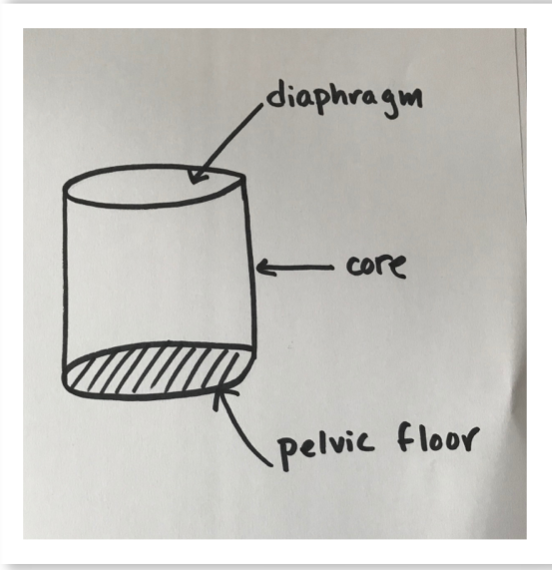
the sides of the canister are comprised of the back muscles and abdominals; they relax and expand on the inhale and contract inward to the axis of the body on the exhale-providing rigidity and support during exertion
the foundation for all of this AND all of the important organs of the lower abdomen is the pelvic floor which relaxes and expands downward on the inhale and contracts upwards on the exhale.
Together the diaphragm and the pelvic floor act like a piston, rising and lowering with every breath to help generate power and strength for the engine that is our body!
The Problem
Individuals recovering from pregnancy and birth OR sufferers of pelvic floor dysfunction, often cannot or do not activate ALL the members of the team when they breath normally or during exertion.
Therefore they have a tendency to hold their breath AND bear down on their pelvic floor and organs in order to feel strong and stable during movement.
And this is a problem because persistent inactivating of OR consistent bearing down on the pelvic floor causes several forms of incontinence, pelvic organ prolapse, pelvic, hip or low back pain and overall weakness of the team that utilizes our breath to stabilize and power the body.
Let’s talk about the role of each member of the team!

1. The core of a mom or body builder with diastasis recti doesn’t generate enough tension on the exhale and therefore can’t offer the support and rigidity that is required for healthy shoulders, strong backs, or a healthy pelvic floor. (Female photo from GirlsGoneStrong.com; male photos from diastasisrehab.com).



2. The pelvic floor of an individual that has recently given birth, has a persistent pelvic tilt and gluteal amnesia (weak glutes = weak pelvic floor) OR pelvic floor dysfunction (see below for stats) isn’t going to function as a piston. It can’t fully relax on the inhale and OR contract as needed on the exhale to provide the stability and support, thus leaving the body susceptible to injuries like pelvic organ prolapse, chronic low back and hip pain, and more. In addition to training the pelvic floor, it is necessary to train clients to neutralize their pelvic position.
When the ribs and diaphragm are aligned over a neutrally positioned pelvis, the diaphragm and pelvic floor are more easily able to work together.
(Photos courtesy of the one and only physiodetective.com


3. The diaphragm of a person with rib flare (often paired with a pelvic tilt) is also not a contributing member of the team because in the flared position, the intercostal muscles of the rib cage never fully relax or contract with the breath, making it difficult to get a full inhale or exhale. The individual is then not fully relaxing or activating his or her pelvic floor. (Photo of male, courtesy of OnlinePhysio.com; pregnant female courtesy of traningfix.com)
The Solution:

When working with my postnatal and pelvic floor rehabilitation clients that have been diagnosed with an inactive pelvic floor or pelvic organ prolapse, we spend A LOT of time both inside and out of the gym re-learning to breath.
First! I teach them to coordinate their pelvic floor and diaphragm with each breath without any weight or exertion. My clients practice this regularly throughout the day in the supine, sitting and standing positions, in order to get all the members of the breathing team coordinated with one another.
Second! Once they’ve had some practice learning to relax the pelvic floor with their inhales and lift it with their exhales, we begin to actively engage the pelvic floor BEFORE any mildly strenuous activities.
I use Julie Wiebte, PT’s cue, Blow before you go to help them trigger pelvic floor activation (aka support!) BEFORE a lift, jump, squat or any sort of exertion takes place.
The “blow before you go” cue tells them to use a tiny exhale to turn on engage their pelvic floor at the beginning of a straining movement and avoid pushing down or holding their breath to complete the task.
So whether we are rolling, bending down to get something off of the floor, getting up off of the floor or a chair, getting in and out of bed, etc. they are using their breath to support them.
With the pelvic floor activated, the body is more stable and the pelvic organs (bladder, uterus and rectum) supported as opposed to pressed downward.
I also program exercise that help my clients work on maintaining stacked alignment of their spine and pelvis and in order to breathe in a manner that recruits the diaphragm, core and pelvic floor to work TOGETHER to generate and release intra-abdominal pressure.
Finally, once they have their breathing pattern down and feel able to support their pelvic floor as needed we add load and then work on dynamic movements like jumps, swings, sprints, etc.
To illustrate the concept, I will show you what this looks like with a kettlebell swing:
Step 1

I address the bell, take a nice deep inhale, expand the rib cage in all 360 degrees. Pelvic floor relaxes down.
Step 2

I hike the bell and release a slight exhale (blow before I go) to activate the pelvic floor to support my core and pelvic organs, let a tiny bit of air out, begin the slow release of my tension breath.
Step 3

As I release my tension breath, I continue to exhale as hard as I need to in order to engage my pelvic floor and create tension in the core to project the bell forward.
It’s really important the pelvic floor clients and postnatal clients learn to use the appropriate amount of tension for the task.
While no tension is a bad thing, using too much tension is ALSO a problem. If this was an 18kg bell and I exhaled super hard and engage the pelvic floor too much or too often, that will eventually lead to a overactive (hypertonic) pelvic floor, which is as problematic as one that is inactive and can present with similar symptoms!
Step 4
I proceed to take a nice big inhale during the downswing and then exhale again to activate the pelvic floor as needed on hip pop…and so on.

I teach my clients to use this very same approach in every day life AND to learn to only dial up as much tension as necessary.
Moving a coffee table is going to require a DIFFERENT amount of tension and pelvic floor engagement than say picking up a bag of groceries will, but BOTH actives should involve the BBYG cue AND start with proper alignment to ensure a full diaphragmatic breath that recruits then WHOLE TEAM!
Takeaways
There are multiple players involved when using our tension breath: the diaphragm (and nearby intercostal muscles of the rib cage), muscles of the core (back and front!) and pelvic floor.
Clients with pelvic floor injuries, diastasis recti, or clients are returning to exercise after having a baby often struggle to effectively activate or relax all of these members at the same time and therefore need training and cues that helps them access the system when necessary to stabilize and protect the body during exertion.
Blow before you go, when coupled with proper alignment a is an effective strategy for helping retrain the brain and the body to recruit ALL of the members of the team, including the pelvic floor during a lift. But it’s important to temper the tension recited during the lift to the task. Heavier weights and harder movements require more tension, while less intense exercise or tasks should still involve only a gentle lift.
If you believe that you may be suffering from any form of pelvic floor dysfunction (see symptoms listed below), consider seeing a pelvic floor physical therapist. Knowing whether your pelvic floor is TOO tight, TOO lax (or a combination of the two) or inactive, is essential for both you and your coach or trainer! Both men and women can suffer form pelvic floor related conditions. You can find your local one here!

Sarah Smith is a personal trainer, level two Russian Kettlebell Instructor, postnatal fitness specialist and pelvic floor and gut health advocate working online and in Raleigh, North Carolina.
She specializes in helping women online and in-person feel strong, confident and capable in their bodies!
Sarah is a mom to three boys and one English Bulldog. She loves soil, coffee and not folding laundry.
Check her out on social media here or get on her email list!! for more content!
More info:
Symptoms of pelvic floor dysfunction include:
A frequent need to urinate. When you do go, you may stop and start many times.
Stress or urge incontinence
Pain in your lower back that cannot be explained by other causes.
Chronic hip pain
Erectile dysfunction (approximately 80% of cases are due to musculoskeletal factors (http://malepelvicfloor.com/sd.html)
Ongoing pain in your pelvic region, genitals, or rectum.
The feeling that you need to have several bowel movements during a short period of time
Prostatitis
The feeling that you cannot complete a bowel movement.
Constipation or straining pain with bowel movements.
Statistics:
Urinary Incontinence ( a symptom of pelvic floor dysfunction) affects 200 million people worldwide. (National Association for Incontinence)
One in four women over the age of 18 experience episodes of leaking urine involuntarily (National Association for Incontinence)
Diastasis recti: 39% of women at 6 months postpartum are still experiencing diastasis recti (diastasisrehab.com)
Pelvic organ prolapse: Research frequently estimates that up to 50% of moms experience some degree of clinical pelvic organ prolapse. There are 300,000 surgeries annually in the US for POP. (https://www.physio-pedia.com/Uterine_Prolapse)
Pelvic Pain: In the United States, estimated direct medical costs for outpatient visits for chronic pelvic pain (women aged 18-50 y) is approximately $881.5 million per year (medscape.com)
Between 8% and 10% of the male population suffers from pelvic pain. But that number is likely higher because studies also show that 50% of men will deal with prostatitis at some point in their lives, and pelvic pain in men is consistently misdiagnosed as prostatitis. (pelvicpainrehab.com)
Find a pelvic floor physical therapist directory
References and further reading:
Bowman, Katy, Mind Your Pelvis, www.NutritiousMovement.com. July 6, 2010.
Bowman, Katy, Diastasis Recti, The Whole‑Body Solution to Abdominal Weakness. 2016.
Cleveland Clinic. Diaphragmatic Breathing. May 2014. https://my.clevelandclinic.org/health/articles/9445-diaphragmatic-breathing.
Gibbons, John. Functional Anatomy of the Pelvis and the Sacroiliac Joint. 2017. Berkeley, CA.
Lee, Diane, Understanding your back and pelvic girdle. 2011. http://dianelee.ca/articles/UnderstandYourBack&PGPopt.pdf
Lo, Antony, “Bulletproof” Your Core and Pelvic Floor – CrossFit East Tamaki, Auckland, NZ – 21/11/2015
Prendergast, Stephen. “Physical therapy for male pelvic pain.” March 2016. https://www.pelvicpainrehab.com/male-pelvic-pain/3805/physical-therapy-male-pelvic-pain-dont-let-penis-come-us/
Wiebe, Julie. The Diaphragm Pelvic Floor Piston Demo,.May 24, 2012. (http://www.juliewiebept.com/video/the-diaphragm-pelvic-floor-piston-demo/)